Every May 23rd, the world celebrates the International Day to End Obstetric Fistula.
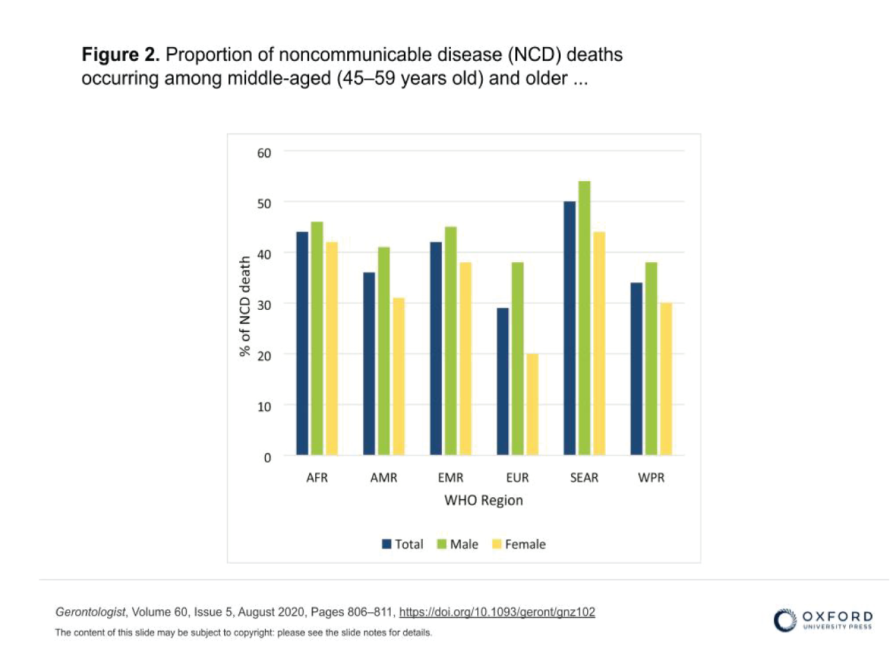
Commonly known as the “disease of poverty,” obstetric fistula (OF) is prevalent in developing countries in sub-Saharan Africa and South Asia – where poverty, inadequate organization of obstetric care, high fertility rates and low status of women in society prevail. WHO estimates more than 2 million young women living with untreated obstetric fistula in Asia and sub-Saharan Africa. There are between 150 and 300 cases per year in Mauritania and nearly 750 cases per year in Niger.
Very disabling, OF is rooted in the perpetuation of traditions such as early marriages, results from weaknesses in the effective support of childbirth and access (both financial and logistical) to emergency obstetric care. A vector of stigmatization, it constitutes a physical and psychological burden for the women who are victims of it.
What psychosocial consequences do these women face? What role do cultural norms, harmful traditional beliefs and practices play in their social exclusion? How does the distress linked to not being taken care of impact the female capital of these countries and what would be the promising solutions at the community level?
Far from being exhaustive, this article exposes the urgency of harmonizing public health policies to eliminate the impact of obstetric fistulas on women, in order to restore dignity to the community (carried by these mothers, by these girls).
- Obstetric fistula: An attack on human dignity
As “the most dramatic consequence of neglected childbirth”, obstetric fistula occurs following a difficult and prolonged childbirth, without medical intervention as soon as possible.
A real public health problem, OF is a perforation between the vagina and the bladder or rectum which results in leakage of urine or fecal matter – creating embarrassment and shame among women suffering from this condition.
Found mainly in rural areas, this disease results from unassisted home births in contexts where accessibility to health structures is a real problem. The low level of formal education within communities, the lack of health awareness, and the lack of education on childbirth and postnatal care constitute major obstacles to the health of mothers and newborns. Increased awareness of the risks of obstetric fistula, as well as better health culture, appropriate monitoring of pregnancies in rural areas, and a demystification of modern medicine could provide women with adequate support and necessary protection.
Social norms play a crucial role in perpetuating gender norms that define the contours of “good” femininity and masculinity. These rigid norms lock individuals into often unchosen social identities, imposing specific expectations and behaviors on them based on their genre. They are reinforced and maintained by individuals and institutions.
Thus, girls are often socialized to be passive and submissive, while boys are encouraged to be active and dominant. These social expectations influence how adolescents perceive their own identity and behavior.
Girls are often valued for their purity and chastity, while boys may be encouraged to explore their sexuality. This differential treatment creates different social pressures around sexual behavior and severely limits women’s choices and opportunities, relegating them to positions of subordination and dependence.
In terms of root causes, OF takes root in social cultures encouraging forced marriage and where women’s status and self-esteem depend almost entirely on their marriage (their relationship with a man) or their ability to have children.
Child and early marriages are often the result of unequal power dynamics, where decisions are made by adults (often parents, without consultation or consent of girls). Families may be motivated by economic considerations, social or cultural, seeking to strengthen family alliances, guarantee financial security or preserve family honor. In Ethiopia, for example, 73% of women aged 45 to 49 were married before their 18th birthday (in 2011); it is estimated that in Niger 76% of girls are married before they turn 18 and there are nearly 68% of girls in the same situation in Chad. We will then speak of “power over” or domination, expressing authority or control exercised by one person or entity over another.
Obstetric fistula then occurs in young women or girls whose body is not yet completely formed, the pelvis not fully developed.. Aged of, at least, 12 -13 years, these young mothers find themselves carrying unwanted pregnancies and risk health complications such as skin infections, kidney problems or even death in the absence of rapid treatment and loss of baby during pregnancy.
However, on a global level, it is estimated that just a 10% reduction in child marriage could contribute to a 70% reduction in maternal mortality and a 3% reduction in infant mortality rates.
To this societal issue is added female genital mutilation which contributes to the growing number of cases of fistula. Perceived as a rite of passage towards femininity and purity, this highly harmful practice for the health of women and girls persists due to social pressure to maintain control over female sexuality.
As highlighted in the Elimination of All Forms of Discrimination Against Women Convention from 1979, “generalized discrimination against women still exists” and “violates the principles of equal rights and respect for human dignity”. The lack of power of a girl/woman to fully decide about her being, her body and their choices constitute a negation of their human rights and an attack on their integrity, their dignity. Subject to gender inequalities, this inferiority complex and this fatalism inscribe themselves in their memory, in their flesh, thus creating a loss of self-confidence and serious psychological after-effects.
For a predominantly female population in sub-Saharan Africa (50.2% in 2022), health needs continue to grow and must be met effectively, in accordance with articles 12 and 14 of said Convention.
Faced with these worrying realities, it is imperative to recognize the profound implications of the deprivation of women’s rights on their psychosocial well-being.
- Psychosocial risks and stigma: The double burden
The women affected by obstetric fistula experience both physical and moral comedown.
Sidelined from the community out of shame and reticence, they find themselves in a situation of extreme economic precariousness (loss of income-generating activity and social weight of cultural norms and exclusion).
Out of shame
Through ignorance of the subject, ignorance of what is happening to them, these women are left to their own devices.
Seen as guardian of family honor, a woman suffering from fistula is perceived as “impure”, leading to her social isolation. Obstetric complications are often interpreted as signs of curse or bad luck, fueling stigma. The woman is expected to bear healthy children and will therefore be rejected by her husband and family in the event of fistula, considering her incapable of fulfilling her duties as a wife and mother. Marginalized, they often lose their place in society, cannot ensure economic activity and are excluded from popular ceremonies and events.
They might then engage in purification rituals and traditional treatments that can aggravate their condition.
By modesty
When a leak occurs, these women avoid social gatherings to escape the embarrassment of being “smelled” or noticed.
This reluctance to be exposed creates a vicious cycle of hiding and social withdrawal. Women feel forced to hide their condition and this social pressure reinforces the taboo surrounding obstetric fistula, creating a climate of silence and censorship. Women find themselves trapped in a cycle where their own dignity and well-being are compromised by societal expectations.
This shame and fear of exposure can lead to a delay in medical treatment and worsen the physical and psychological complications associated with obstetric fistula.
Involving husbands as valuable support in women’s recovery process is crucial to alleviate the social distress, depression, and anxiety they face. The family plays an essential role in these women’s journey towards healing, as well as in their access to repair and social reintegration. It is essential that traditional and religious leaders understand and support the need for women to be cared for.
- Urgent response for maternal health : Community solidarity at the heart of recovery and reintegration initiatives for women injured by OF
Although surgical repair can significantly improve their quality of life, it is not always enough to overcome the resulting emotional after-effects of fistula.
Beyond strengthening the resilience of these women, it is important to address the root causes to prevent and no longer cure. The exercise of power is an important aspect of relationships. The more power a person has, the more choices they have.
The empowerment of women affected by OF is of paramount importance in their journey of healing and reintegration into society. “Power from within”, which encompasses strength, resilience and individual autonomy, becomes an essential lever in this process.
This power to centralize one’s own subjectivity, far from preconceived norms of femininity and masculinity, thus becomes essential. By giving women victims of obstetric fistula the tools they need to rebuild their lives, we help them regain control of their destiny.
If African governments are committed to improving maternal health by investing more in universal health coverage and making prevention and treatment of obstetric fistula accessible, a focus on the community component is essential.
The full involvement of families and communities is essential in this process to eliminate taboos, superstitions and ignorance on the subject, in order to promote compassion and solidarity towards these women. “Power with” is then established and refers to the ability of individuals or groups to work together in a collaborative and supportive manner to achieve common objectives.
In this context, women, families, communities and health professionals must join forces to end stigma and discrimination, and to promote access to appropriate and respectful health care.
It is crucial that communities understand that exercising responsible sexuality does not contravene religious and cultural principles, but rather demonstrates a true understanding of parenthood and the responsibilities that come with it, as well as mutual respect. By educating communities about sexual and reproductive rights, implementing awareness-raising programs and encouraging open dialogue, it is possible to create an enabling environment for women’s health and well-being.
To achieve this goal, several urgent actions are necessary:
To raise awareness
- Organizing awareness workshops in villages to provide information on the causes, consequences and available treatments for obstetric fistula. Members of village committees as in Guinea, chosen by local leaders, can facilitate these discussions.
- Using testimonies from survivors would help demystify the condition and reduce stigma. Added to this is the use of community radio, posters and street theater to share educational content.
Strengthen community solidarity
- It is important to highlight community leaders and religious leaders supporting the cause to influence public opinion positively
- Women victims of OF should benefit from local support groups where they can share their experiences and get emotional support.
Regular meetings led by health professionals and psychologists would be organized to ensure emotional and psychological monitoring of these women.
Through waiting homes and rehabilitation centers, they will benefit from regular essential care and rest.
Support economic and social reintegration
- Initiate microfinance projects would help women start small businesses, to support themselves and their families. Training in business management and financial skills would follow to ensure mastery of their business.
- Creating artisanal cooperatives for the production and sale of handmade items would also contribute to the artisanal influence of our countries.
Together, these actions are much more than just measures.
They represent a cry for justice, an affirmation of the value and dignity of every woman affected by obstetric fistula.
They reflect a collective desire to put an end to silent suffering and marginalization, to give these women their rightful place in society. Every voice counts, every story must be heard.
Their emotional well-being is fundamental to their autonomy and essential for the development of our countries.
BIBLIOGRAPHY
- BBC Africa. “Obstetric fistula: the disabling pathology of the poor”. February 5, 2019
- Studio Kalangou. “Health: causes and management of obstetric fistula”. June 23, 2021
- Diallo, AB; Sy, T et al. “Obstetric vesicovaginal fistulas in Guinea: analysis of data from 3 treatment sites of the NGO Engender Health”. February 2016.
- UN News. “In Niger, women with fistula find care and comfort in health centers.” July 8, 2018.
- UN Senegal. “The United Nations Population Fund (UNFPA) listens to community talks on eliminating obstetric fistula by 2030”. August 14, 2023.
- Cook, Rebecca, J. “Women’s Health and Individual Rights.” WHO, 1995
- OHCHR. International standards on the right to physical and mental health.
- Mbacké Leye, Mamadou M; Ndiaye, Papa et al. “Sociodemographic factors and management of obstetric fistulas in the South-East of Senegal”.
- Delamou, Alexandre; Douno, Moussa et al. «Stakeholders’ perceptions on improving women’s health after obstetric fistula repair: results from a qualitative study in Guinea». African Journal of Reproductive Health August 2022
- Ndiaye, P; Amoul Kini, G et al. “Project of the woman suffering from obstetric fistula in Niger”. Tropical medicine, 2009
- https://gallica.bnf.fr/ark:/12148/bpt6k6443399c/f63.item
- Lufumpa, Eniya K et Steele, Sarah. « Obstetric Fistula: A Narrative Review of the Literature on Preventive Interventions in sub-Saharan Africa ». African Journal of Reproductive Health September 2016
- Tripathi, Vandana et Mallick, Lindsay. « The association between female genital fistula symptoms and gender-based violence: A multicountry secondary analysis of household survey data ». Tropical Medicine and International Health. 2018
- Ntchapda, Arnaud. “In sub-Saharan Africa, the difficult management of obstetric fistulas”. Hello Doctors Africa. January 19, 2023
- Fall, Aida Ndiaye. “Obstetric Fistula: “In sub-Saharan Africa nearly 2 million cases recorded and less than 500 cases per year in Senegal”, (Urologist)”. Dakar News. May 14, 2024
- Dakar News. “Care for women with obstetric fistulas in Senegal: the MSAS announces universal health coverage from 2023”. December 30, 2022
- Guinea Morning. “Obstetric fistula: “some patients are rejected by their families”, deplores Dr Mamoudou Doumbouya”. September 14, 2023.
- UNFPA. “End fistula today: invest in quality health care, empower communities.” May 26, 2022
- Guinea Morning. “Prevention against obstetric fistula: “We must avoid early marriages”, advises Dr Ben Youssouf Keïta”. May 10, 2024
UNFPA. “I only want one thing: to be cured of fistula.” May 23, 2020.
https://senegal.unfpa.org/fr/news/%C2%AB-je-nai-quune-seule-envie-gu%C3%A9rir-de-la-fistule-%
- UNFPA. “Obstetric fistula”.
- OMS Africa. “Female genital mutilation in Senegal: a multi-actor struggle for lasting change”. March 4, 2024
- Humanium. “Child marriage in sub-Saharan Africa: the case of Niger”.
December 1, 2020
- Excision, let’s talk about it! “the figures of excision”.
https://www.excisionparlonsen.org/niger/ - FranceTV. “Guinea: Kadiatou fights against early and forced marriages”. December 17, 2020.